 The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.
The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.It was written in german and was translated into more than 10 languages already. German is not freely available, as the rights are held by a publisher, but all these translations are available as ebooks / PDFs for free, as a gift of Björn for you, for the New Earth, for a new time.
In cooperation with Björn, it is splitted on "Disease is Different" into the sections by organ systems and combined with the real cases of our international testimonial / report archive of the related organ system.
TEETH AND JAW
Every tooth is made up of a dental crown (corona dentis), a neck (colum dentis) and a root (radix dentis). What we see externally in a healthy set of teeth is only ectodermal tooth enamel, which covers the mesodermal dentin lying below it like a glaze. In turn, the dentin covers the and nerve and vessel-filled tooth pulp (pulpa).
The tooth enamel consists of 97% inorganic components (crystals). It is formed exclusively during tooth development by so-called ameloblasts.
These ameloblasts exist only during tooth development. After the tooth is “out,” the enamel is finished like a perfect crystal and the ameloblasts die.
Dentin consists of 70% inorganic material (calcium hydroxyapatite), 20% organic collagen and 10% water.
Since dentin and enamel are largely composed of crystals (minerals), fully developed teeth follow the laws of inorganic chemistry.
Dentin and enamel also do not have any cells that can carry out cell augmentation and cell degradation, like the bones do with the so-called osteoblasts and osteoclasts.
The teeth, according to Dr. Hamer,
function like the rest of the body, strictly according to the 5 Biological Laws of Nature. He also applied the germ layer SBS patterns to the teeth and derived the following conflict contents from the teeth’s tasks.
Both incisors: not being able to or allowed to bite, snap, or bare one‘s teeth. Canine teeth: not being able or allowed to sic, seize, capture, or hold onto. Bicuspids: not being able or allowed to chew. Molars: not being able or allowed to grind.
On the huge “Tooth Table of the Germanic New Medicine” he described, among other things, the SBSs of the enamel and dentin.
However, based on my 15 years of experience and the experience of dentists who are supportive of the New Medicine, enamel and dentin function according to this pattern only while the teeth are developing.
That’s why I had to completely rewrite this chapter.
I could not continue to support a theory that did not hold up in practice.
Taking this step – a paradigm shift back to conventional dentistry – was not easy for me.
I would like to thank the dentist, Dr. Isabella Pfaff, who provided me with significant insights.
How do cavities form?
Local demineralization of the enamel or dentin. This is caused by an acidic oral milieu or the acidic excretions of bacteria.
The decisive factors for healthy teeth
Alkaline milieu
After the tooth is “out,” the enamel solely dependent on the chemical balance in the mouth, or more precisely, on the electrolytes in the saliva:
Ideally, saliva is predominantly neutral to basic.
During the day, however – especially after meals – the pH of saliva is acidic. This causes minerals (alkalis) to be dissolved from the teeth (= demineralization).
At night or during periods of rest, this dynamic is reversed: The saliva, which is now alkaline, supplies the teeth with new minerals > balancing the demineralization-remineralization balance > healthy teeth.
This balance only works through a permanent alkaline boost (more on p. 65).
During the day, you can reduce the demineralization of the teeth by “interval fasting”: The longest possible interval between meals keeps the “acid flood” to a minimum.
Interestingly: Herbivores spend most of the day eating – in terms of teeth, they can afford to do so because leafy greens are some of the most alkaline. Carnivores, however, eat meat (acid-forming) only once a day – if at all – (“interval fasting”).
In his book, “Healing Toot Decay” (see source list), Ramiel Nagel shows us that the tooth decay has gone hand in hand with the introduction of modern industrial food. From his perspective, cavities also come from malnutrition and stress. A very brief summary of Nagel’s nutritional recommendations for the regeneration of teeth and gums:
• Avoid acid-forming foods like sugar (e.g., in cakes, chocolate, soft drinks, sweet fruits), isolated starches (white flour, bread, pasta). These short-chain carbohydrates cause blood sugar spikes that disrupt the calcium-phosphate balance. Also avoid oxalic acid and phytic acid.
• Give preference to natural foods rich in vitamins. Especially important: natural calcium and phosphate (e.g., in vegetables, unpasteurized dairy products, fish), naturally bound vit. A, D, C (e.g. in cod liver oil (see p. 68), fish, eggs, unpasteurized butter, cream, cheese, avocado, herbs, vegetables).
Oral hygiene, brushing teeth
All of the New Medicine dentists I have interviewed say that hygiene, care, and healthy food are all crucial to healthy teeth.
This involves the removal of soft dental plaque – a biofilm made up of food residues and bacteria.
Most plaque is found in the interdental contact areas, in the crevices (fissures) of the chewing surfaces and in the spaces between the teeth and the gums (sulcus).
Cavities develop mainly in these recesses, and almost never on smooth, easily accessible tooth surfaces.
Dental plaque envelops the tooth in a coating of acid (excretory products of bacteria) and prevents nighttime remineralization because the enamel lacks direct contact with saliva.
The fact that bacteria only multiply in a carbohydrate-rich environment underlines the importance of good alkaline nutrition.
With good care, bacteria cannot “hold on,” even in recesses and their acid excretions cannot corrode holes in the teeth. Of course, enthusiasts of the 5 Biological Laws like to point out that animals do not practice dental hygiene in nature. Yes, but wild animals don’t snack on junk food; they exercise their jaws and regularly put their teeth to the test. Also, they are not constantly suppressing their impulses to bite other animals.
• I personally brush my teeth with a salt solution (sea salt or Himalaya salt dissolved in water and stored in a bottle or glass jar). I take a tablespoon of salt solution into my mouth and brush my teeth as usual. If the gums are sensitive, one can dilute the solution at the beginning.
• Cayce: Brush the teeth with a solution of bicarbonate of soda and table salt.
• New Medicine dentists recommend using fluoride-free toothpastes.
• Brush your teeth 2 times a day and use dental floss or an interdental brush once a day.
• Every once in a while, oil pulling with sunflower oil (see p. 68).
• Regular dental checkups by a dentist.
Exercise
Our entire organism depends on sufficient movement, and this also goes for the metabolism in the jawbone, gums and root canals: Movement improves the supply of nutrients and O2 and the removal of CO2 and metabolic waste products. Of course, the blood and lymphatic systems need regular movement for good circulation.
The direct effects of exercise: With walking/running/gymnastics, the oral mucosa and tongue rhythmically glide over the surfaces of the teeth. In the process, the teeth receive optimal care and are remineralized by the (ideally alkaline) saliva.
If teeth remain partially dry for several weeks (e.g. when a seriously ill person lies with their mouth open), they will decay. Also, people breathing through their open mouth at night (so-called mouth breathers) will also have partially dry teeth and this is a known cause of tooth decay.
Teeth are there for biting and chewing
If we use our muscles, they stay strong. If we move our joints, they stay intact. If we let our teeth regularly break down whole carrots, we will be pleased with our strong teeth.
When we constantly let squishy hamburgers slide down our throats, we are insulting the “pearly heroes” in our mouths.
It is similar with the jaw: A child who chews properly forms large, strong dental arches. > Large dental arches provide enough space for ALL teeth – including the wisdom teeth.
Today, when wisdom teeth need to be extracted due to a lack of space, this is not fate; it is a “homemade” situation.
Psyche
Stress makes all bodily fluids acidic – including saliva. Relaxation/peace/joy makes you alkaline – and this can be measured in saliva by means of pH indicator strips.
Constant conflict activity (see p. 24) damages our teeth, because their remineralization cannot keep up with their demineralization (see p. 224).
Without a doubt, the bite conflicts described by Dr. Hamer (see p. 223) definitely have an influence on the health of our teeth: on the tooth nerves, dentin forming odontoblasts in the root canal, periodontium, and oral mucosa (see p. 226f).
In my experience, argumentative people tend to have good teeth. I.e., they do not shy away from confrontation and they speak their mind freely (the opposite of diplomats). Therefore, a decisive factor in the healthy development of teeth (during the period beginning 40 days after conception up to the age of 16), is an ability to handle bite conflicts well. This goes for the mother, the father, and the child themselves. A good atmosphere of constructive debate, an ability to acknowledge aggression, and understanding that you don’t always have to bite your way through (you can also take it easy) will lead to beautiful teeth.
Our basic tooth structure is usually similar to one of our ancestors (see conditioning, family waltzes, p. 30).
Frequently asked questions
So having bacteria in your mouth is bad?
Yes and no. Bacteria are omnipresent in the oral cavity (we have identified approx. 500 species). The decisive factor is which bacteria make up our mouth’s “microflora society.” Claude Bernard’s saying that, “The microbe is nothing, the milieu is everything,” is as true for the mouth as it is for everywhere else in the body.
Each species of bacteria can only thrive where the milieu is right for it.
The general rule: the more nutrients, the more bacteria. Also, the lower the milieu’s O2 content, the more problematic the bacterial species. The main food source of acid-excreting bacteria is carbohydrates – which are dissolved in saliva and deposited in recesses.
Poor diet, stress, and a lack of exercise will alter the oral flora. Bacteria with neutral excretions will be displaced by colonies of bacteria with highly acidic excretions (e.g., Streptococcus mutans).
These bacteria are indeed a problem, but they are not the cause.
Why do toothaches hurt the most when we are resting?
During periods of stress/daytime, we hardly notice cavities or bacterial colonies (dental foci, e.g. in the nerve canal). However, during vagotonia/at night, inflammation occurs due to blood vessels dilating and an increase in body temperature and metabolism. This leads to swelling and increased tissue pressure. At the same time, more acids are produced in the local area of inflammation. Together, all of these factors cause pain. A toothache at rest can mean that bacterial growth is “smoldering under the surface.” Pain can also occur after stress, when a tooth was put under too much strain (irritation of the root membrane) – in this case, you can wait and see if it subsides.
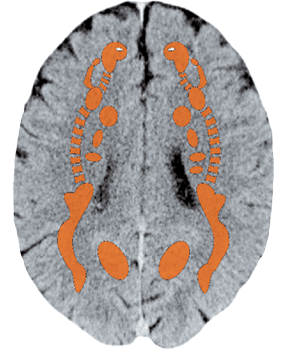
What purpose do the tooth relays (HFs) in the brain serve?
I assume that the relays discovered by Dr. Hamer for the dentin and enamel are only in play during the development of the teeth, i.e., only during the time when the hard substance of the tooth is being formed. When the “mouth crystals” (teeth) are fully formed, the brain impulses are no longer coupled.
Should I wait if I have a cavity?
No, because larger cavities will not fill up again by themselves. Cavities are perfect recesses for collecting residues – an ideal habitat for bacteria. If the cavity is not filled quickly, acidic secretions from bacteria will continue to make it larger and deeper. When it reaches the nerve canal, the party’s over. At that point, a root canal is usually the only treatment that can help.
What happens when you don’t do anything about a cavity?
If you change your diet and stick to it, do a lot of exercise in the fresh air, take optimal care of your teeth (brushing your teeth & especially the cavity with a single tuft toothbrush), consistently resolve bite conflicts, and maintain inner peace, you may stop small cavities from getting larger. They may also harden a little from the inside (through remineralization), but they will remain an unsightly dark color. However, even if you do all that, the chances of a cavity getting larger are still high.
Where can we expect recovery?
• In the jawbone and gums.
• In the tooth structure (enamel, dentin) through saliva remineralization, only when cavities are very small.
How can I recognize a good dentist?
Fairness (recognizable by fair rates + minimally invasive procedures) and accuracy (a certain perfectionism, recognizable by the time they take) are the most important qualities of a good dentist. Cheap and fast usually mean that you will be paying for even more work in the future.
Should I go to the dentist for check-ups?
Yes, because small cavities are easily filled. This means that only a small amount of the tooth’s substance will be lost. In the case of consistent, increasing pain, you shouldn’t wait, because the pain usually only begins when the cavity is already approaching the nerve canal. The later you react, the more work it will take to repair.
What is the significance of dental foci?
Unfortunately, the New Medicine has not paid much attention to dental foci (bacterial colonies in the teeth) so far. Dentists and naturopaths agree that bacterial foci poison the body from within (bacteremia). The severity of their effect depends on the size and number of the foci and the vitality/robustness of the individual. For people with poor excretory function, e.g., active kidney collecting tubules (see p. 277ff) or a tendency to constipation, dental foci are doubly unfavorable. (TN: Curiously, a 1993 study by Bieniek and Riedel concluded that (in males), “a direct causal relationship exists between bacterial colonies (dental foci) and therapy resistant bacteriospermia which probably leads to subfertility.” Six months after the study’s test group underwent dental treatment, “about two thirds of the spermiograms proved sterile.” (i.e., bacteria was no longer present). “Spermatlogical parameters, such as motility, density and morphology, had also clearly improved.”)
Which filling/crown is the best?
All decent dentists will try to preserve as much of every tooth as possible and only drill out what is necessary. Of course, mercury-amalgam fillings should be avoided. For extra-sensitive people, individual kinesiological testing can help determine which material is best for you.
Jawbone
Self-esteem conflict,
not being able to bite
Oral Mucosa
(non-keratinized
squamous epithelium)
Illustration based on the image in Dr. Hamer’s Scientific Table of the New Medicine, cover p. 3, top right, Amici di Dirk Verlag
Tooth Neck
Tooth Enamel
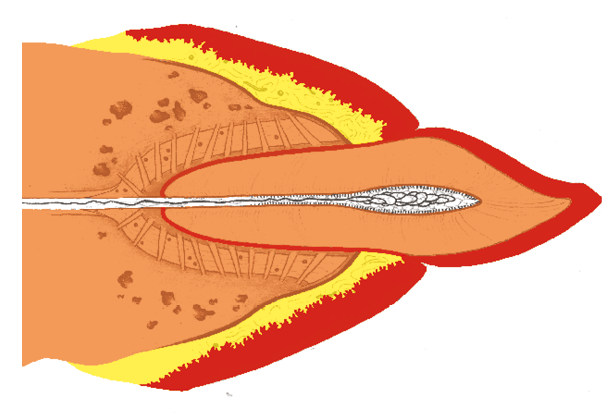
Tooth Dentin
Gap between tooth and gum (sulcus)
Cementum
Oral Submucosa
(according Dr. Hamer)
Periodontal disease (atrophy of the gums)
Receding gums used to be called periodontitis, today, periodontal disease. However, it is in fact bone atrophy (tooth socket atrophy), since the gums merely cover the bone.
This hardly ever affects young people, but most people are affected after a certain age. Thus, it is a disease that accompanies age, but also civilization!
A good connection (attachment) between the tooth and gum is crucial. The formation of gum pockets (gingival sulcus) is typical of periodontitis: When pocket depth exceeds 4 mm, dentists start referring to this as periodontal disease.
It usually begins around the molars and at the edge of tooth crowns (largest recesses for residue). This is also where the “trail blazers,” plaque and tartar, are most commonly found.
If gums are chronically inflamed for years, the bone makes room, i.e., it shrinks > the tooth anchorage (root membrane/Sharpey’s fibers) becomes loose, the tooth becomes wobbly, and may ultimately fall out.
Chronic inflammation/bacterial foci pose a problem for the body: With a flood of countermeasures, the body tries to clean up foci. In the end, however, the body’s own tissue also suffers when masses of white blood cells and enzymes are brought into play (the body’s own tissue is “melted down”).
In addition to these biochemical-mechanical causes, the following conflicts are also likely to play a role:
| Conflict | Self-esteem conflict of not being able to bite, to defend oneself, or to assert oneself. Not being able to bite your way through a situation. |
|---|---|
| Example | a A 46-year-old cheats on his wife and pays for it with prostate cancer. (See: p.316). That is not all: after he confesses to his wife, she becomes, understandably, distrustful. She wants to go everywhere with him and is always checking up on him. The patient feels guilty toward his wife and no longer dares to be demanding. He accepts all the limitations placed upon him = active self-esteem, bite conflict. > Subsequently, he develops extensive, advanced parodontitis, the upper jaw being affected more then the lower jaw. His once white teeth become discolored and are now yellowish-gray. In addition, the dentist finds a decrease in their vertical dimensions (the teeth have sunken). A root planing is carried out. Therapy: When the couple sees the connections, they decide that they should renew their marriage vows with a little ceremony – from now on, he will remain faithful and she puts an end to the whole matter in her mind. Two years later : the relationship is rosy again and the patient’s teeth are solid again. (Archive B. Eybl) |
| Conflict-active | Degradation of the tooth socket (dental alveolus), especially near recesses. The neck of the tooth appears longer because the periodontium is shrinking = periodontal disease. No pain.. |
| Repair phase | Inflammation, bleeding (while brushing), pain, restoration of the gum. Please note: We should face the facts – If the inflammation lasts longer than two months, it most likely has a biochemical-mechanical cause (see above). |
| Bio. function | Strengthening of periodontal (tooth anchoring) apparatus. |
| Therapy | Determine the conflict and conditioning and, if possible, resolve them in real life. Guiding principles: “I am strong and brave!“ “I‘ll bite if necessary!“ Imagine the situation or the adversary and bite with satisfaction. Alternate strategy: forgiveness. Think positively about your teeth and picture them being healthy and shiny. Have a dentist or dental hygienist clean the gum/tooth pockets with curettes: Plaque is cleaned from the tooth root surfaces as thoroughly as possible and the pockets are rinsed with special disinfectant.. At the same time, you should eradicate any bacteria that may have penetrated the gums (sample taken beforehand + laboratory examination) with a suitable antibiotic. Alternatives: MMS (see p. 68). Improve brushing/mouth hygiene, use interdental brushes, and continue brushing even if your gums bleed. Fortunately, surgically removing gum pockets is hardly ever practiced anymore. Establish an alkaline milieu in your mouth: Put sodium bicarbonate powder in your mouth every so often or gargle with this in solution if necessary. Stop smoking. See also: Decisive factors for healthy teeth above. Bach flowers (see p. 59): larch, centaury. Lymph drainage massages (see p. 68), oil pulling (see p. 68). Tea/mouthwashes: comfrey, horsetail, possibly restharrow, chamomile. Xylitol, MMS (see p. 68). DMSO. Rinse mouth with salt water, EM, colloidal silver. Hydrogen peroxide. Natural borax – hold in mouth before swallowing. Cayce: for susceptibility to parodontitis and cavities, clean and massage the teeth and gums with ipsab powder (= prickly-ash, North American “toothache tree“). |
Gingivitis and parodontitis – inflammation of the gums, parodontium
Always found at the beginning of periodontal disease (see p. 226), usually gum bleeding at the same time (= warning sign).
If an SBS is primarily or partly involved:
| Phase | Repair phase. Restoration of the mesodermal gum tissue. Therapy see p. 226. |
|---|
Gum proliferations (gingival hyperplasia, epulis)
Possible causes:
• Parodontal disease (see p. 226f) can turn into a gum overgrowth.
• Poorly positioned (disturbing) dentures (braces) or crowns: chronic inflammation from friction with the dentures > proliferation of the gums.
• Side effects of medications: Especially epilepsy drugs, immune suppressants, blood pressure drugs (calcium channel blockers).
If an SBS is primarily or partially involved:
| Phase | Persistent repair. Exaggerated restoration of the mesodermal gum tissue. |
|---|---|
| Therapy | According to the cause and the measures described on p. 226 f. OP as necessary. |
Jaw Tumor (odontoma, myxoma, osteosarcoma)
| Example |  A 50-year-old, married, right-handed woman fulfills her long-time dream: With a considerable sum (her entire savings), she opens a flower boutique together with a partner. Now, she is self-employed. Unfortunately, her project turns out to be a mistake, because shortly after opening, there is a dispute with the landlord. The business also doesn’t take off as hoped. = Bite conflict – she would like nothing more than to tear the landlord to shreds and she isn’t succeeding professionally. After two years, she finally pulls the emergency brake, leaves the partnership and writes off the money. = Beginning of the repair phase: She experiences tooth and jaw pain (right side) and chronic fatigue. When the pain doesn’t improve, she is taken to the hospital where a jaw tumor is diagnosed. An operation follows immediately. (Archive B. Eybl) A 50-year-old, married, right-handed woman fulfills her long-time dream: With a considerable sum (her entire savings), she opens a flower boutique together with a partner. Now, she is self-employed. Unfortunately, her project turns out to be a mistake, because shortly after opening, there is a dispute with the landlord. The business also doesn’t take off as hoped. = Bite conflict – she would like nothing more than to tear the landlord to shreds and she isn’t succeeding professionally. After two years, she finally pulls the emergency brake, leaves the partnership and writes off the money. = Beginning of the repair phase: She experiences tooth and jaw pain (right side) and chronic fatigue. When the pain doesn’t improve, she is taken to the hospital where a jaw tumor is diagnosed. An operation follows immediately. (Archive B. Eybl) |
|---|---|
| Phase | Repair phase or persistent repair (recurrent conflict), possibly with syndrome. Restoration of the jawbone after previous cell degradation. Severe pain. |
| Therapy | The bite conflict is resolved, support the repair phase. If recurring, determine and resolve the conflict, conditioning and beliefs. If necessary, resolve refugee crisis. Change diet (see: p. 224). Attention: Do not puncture > danger of callus leakage > resulting in a “sarcoma.” Lymph drainage (see p. 68). See also: repair phase at the brain level, p 67. |
Jaw cysts
| Phase | Recurring–conflict, usually with syndrome. Restoration and degradation phases repeat themselves > formation of hollow spaces (cysts). If a jaw cyst is discovered by chance after an x-ray, it is possible that the SBS had taken place quite long ago and is “over and done with.“ |
|---|---|
| Therapy | Determine and resolve the conflict, conditioning and belief (system). Change diet (see: p. 224). |

Grinding of the teeth (bruxism)
Some of us have taken the words “Clench your teeth!“ too literally. Teeth-grinding is usually noticed only by the partner because it occurs in the context of repair phase crises during deep sleep.
The grinding wears the teeth down unnecessarily, therefore, something should be done about it.
| Conflict | Motor conflict: not being able or allowed to snap, grind or “bite one’s way through.” One believes that they must bite their way through. Issues: doggedness, uptightness, fanaticism. |
|---|---|
| Example | ➜ During the day, someone wishes to bite often, but does nothing, because they are too cowardly > at night they enter the repair phase and grinds their teeth during repair phase crises. At night, one does (biting) what they didn’t do during the day. |
| Phase | Repair phase crisis in the context of the repair phase > cramping of the jaw muscles (masseter, temporal, medial pterygoid) during relaxation (at night) – teeth-grinding = “chewing muscle epilepsy.“ Usually a recurring–conflict. |
| Questions | Grinding since when? (Ask partner, parents. A bite conflict has been ongoing at least since then). If it was especially heavy: What happened the day before? (Indication of the conflict). How is it on vacation? (If better > conflict in daily life). Ancestors/family members also affected? (If yes: work out the family issue). |
| Therapy | Find out what the conflict and conditioning are and, if possible, resolve them in real life so that the persistent repair comes to an end. Guiding principle: “No more ‘grin and bear it.’ If need be, I‘ll bite!“ Imagine the situation or the adversary and bite. Immediately address everything bothersome or what one disagrees with and then bury it. Thereafter, reconcile with the situation internally or personally with the person in question. Bach flowers (see p. 59): agrimony. Occlusal bite block/splint (“night-guard“), so the teeth don‘t get worn down grinding in the night. |

Molar incisor hypomineralisation, MIH
In this congenital disease, the enamel is partially missing from molars and incisors.
How it looks: whitish-yellow to yellow-brown discolorations with a rough surface that are sensitive to touch.
Tooth enamel is formed exclusively by ameloblasts during tooth development. This happens during the period from 40 days after conception until the age of 16 – therefore, this is caused by a massive bite conflict (see p. 223) in mother or child during this period.
Possibly also extreme malnutrition in mother or child.
Therapy: CM care.
Periodontal abscess (tooth fistula)
Here we are talking about accumulations of pus in the gums. According to Dr. Isabella Pfaff, there are two types in practice:
• Abscesses, coming from foci at the root tips of dead teeth.
• Abscesses, from foci in deep gum pockets in the context of periodontal disease.
Therapy: Cleaning of the foci, treatments on p. 226.
Dental calculus (tartar)
= calcified plaque. Some are prone to it, some are not.
• Most frequently in the area of the salivary gland openings = indication of calcium-saturated saliva which tends to crystallize (unfavorable mixture of secretions).
• In the context of periodontal disease (see p. 226f), inflammatory excretions crystallize at the tooth necks (so-called calculus or tartar).
• Conflict: More calculus is formed in the area around loose teeth = hanging conflict of periodontium or jawbone > callus enters the oral cavity from gum pockets. This “liquid bone mass” (mixed with plaque) hardens on tooth necks = calculus.
Therapy
• Mechanical removal, regular dental prophylaxis.
• Improve dental hygiene and nutrition, regular exercise (see p. 224).
• If nothing is done, new recesses will develop between the tartar and gums > periodontal disease.
Misaligned teeth (malocclusion)
Dental arches too small (too little space for teeth):
Underdeveloped jaws are usually under-challenged jaws (see “Teeth are there for biting and chewing” p. 224).
According to Dr. John Flutter, an incorrect “swallowing pattern” is the cause of most malocclusions. The infant swallowing pattern is characterized by negative pressure in the mouth generated by the sucking reflex. The infant must create this negative pressure by tensing the cheek and lip muscles.
After infancy, a change naturally occurs: From then on, the tongue should rest against the palate while swallowing, without the lip and cheek muscles moving.
Through the use of pacifiers or by copying the incorrect swallowing pattern of adults, this can make the changeover to the correct, “adult swallowing pattern” more difficult.
If the tongue presses against the palate during swallowing, the upper jaw can develop well in terms of size.
However, if the tongue lies in the lower jaw while swallowing, the upper jaw does not receive sufficient growth impulses. This results in what is called “narrow jaw.”
Here, the lower jaw is not pronounced enough, it is too small in relation to the upper jaw.
Cause: Tension of the lower lip muscles during swallowing > the lower lips press against the lower incisors and the lower jaw.
Psychic components: lower jaw + teeth form our profile: not being able to show an angle, introverts.
Here the lower jaw is oversized in relation to the upper jaw. Underbite occurs when the child gets into the habit of pressing the tongue against the lower incisors when swallowing.
Psychic components: One shows their profile/angle, tend to be extroverted people.
Therapy
• Show the child how to swallow properly: tongue on the roof of the mouth, lips not moving, tip of the tongue not in contact with incisors.
• Do not provide a pacifier.
All experience reports on the organ system “Teeth and Jaw” from the International Report Archive:
| Author | Title and Overview | Keywords | ||||
|---|---|---|---|---|---|---|
 | 2025/08/28   The way symptoms in a small child could be used to find out the mother's primal conflicts. | Experience report: teeth grinding and enuresis, as well as cerebellar constellation | ||||
 | 2025/04/28 When my boss yelled at me, I had toothache for hours afterwards when eating and rinsing with cool water (as if there was a hole in my tooth) .. | |||||
2024/12/19 Around December 2023, I noticed that I felt slight pain when biting on my right side. Then it got worse and worse over the months until I couldn't bite on that side at all from around May ... | ||||||
 | 2021/06/17  On the afternoon of the second Friday in January 2004, a sudden severe toothache began in a molar on the lower right side; the pain was permanent. | |||||
| 2015/01/01 Here is a list of other sources where experience reports with the 5BN can be found, e.g. to:: Bursitis, conjunctivitis, rheumatism, diabetes, hay fever, psoriasis, bedwetting, stuttering, oceans, aggressive constellation, endometrial CA, cervical cancer, shingles, tinnitus, toothache, heart attack, high blood pressure, colic, slipped disc, knee pain, leukemia, bone cancer, voice gone, stomach pain, hives, Epilepsy, intolerances, Crohn's disease, skin rash, facial paralysis, hiccups, anorexia, bronchitis, corneal inflammation, migraine, thyroid cyst, aphthae, osteolysis, gastritis, rectal spasms, milk duct carcinoma, allergies, hepatic coma, gray hair, nail fungus, heartburn, nasal polyps, caries, heart attack, ankylosing spondylitis, melanoma, psoriasis, water belly, hailstones, prostate, . .. |