 The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.
The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.It was written in german and was translated into more than 10 languages already. German is not freely available, as the rights are held by a publisher, but all these translations are available as ebooks / PDFs for free, as a gift of Björn for you, for the New Earth, for a new time.
In cooperation with Björn, it is splitted on "Disease is Different" into the sections by organ systems and combined with the real cases of our international testimonial / report archive of the related organ system.
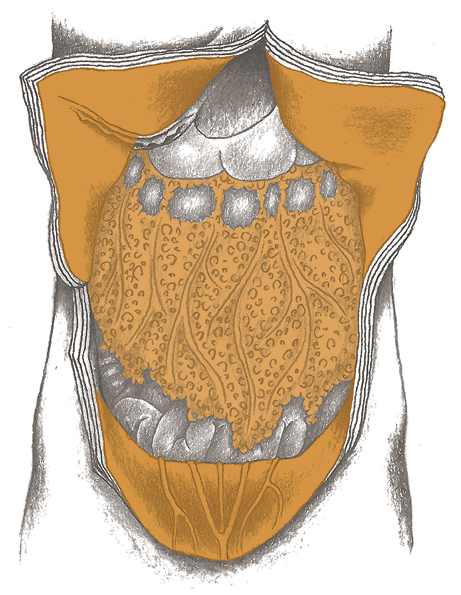
PERITONEUM, NAVEL, GR. OMENTUM AND ABDOMINAL WALL
The abdominal cavity is lined with the peritoneum, which is entirely composed of mesodermal tissue.
There are two layers:
The outer (parietal) layer is attached to the abdominal wall, the inner (visceral) layer forms the outer cover of the organs.
There is a lubricating fluid in the wafer-thin space between the two layers, which allows the organs to slide about.
The greater omentum is an apron-shaped fold of the peritoneum that is attached to the stomach and colon and hangs forward over the winding small intestines.
It can move around on its own, so that it can purposefully lay itself around centers of inflammation in order to isolate them. For example, it folds itself over a ruptured appendix to keep the contents of the intestine from entering the abdominal cavity.
Peritoneum
Attack against
the abdomen
Abdominal Wall
Self-esteem conflict,
issues: pushing/pressing
Greater Omentum
Conflict related to
the abdomen

Cancer of the peritoneum (peritoneal cancer, peritoneal mesothelioma)1
| Conflict | Attack-to-the-abdomen. Actual attack, threat, or perception of an attack. Fear that something is wrong with the abdomen (intestines, stomach, liver, pancreas). |
|---|---|
| Examples | ➜ Very often due to brutal diagnoses like: “You have a lung tumor,“ or “You have a malignant breast cancer. We will have to operate at once.“ ➜ Evil words, insults, or verbal abuse, can be felt as blows or injuries. ➜ Intense abdominal pain, regardless of where it comes from (colic, poisoning, etc.) can also be felt as attack conflict > cell proliferation in the active-phase, cell degradation in the repair phase.  A colon cancer tumor, 17 cm (6.7 in) in diameter, is diagnosed in a 69-year-old woman. Considering the size of the growth, the prognosis is very unfavorable = attack against the abdomen. The patient feels threatened by the gigantic tumor in her abdomen > growth of cells in the peritoneum = peritoneal cancer. Three weeks later, as the tumor is removed, the surgeons find a number of stipple-shaped mesotheliomas. (Archive B. Eybl) A colon cancer tumor, 17 cm (6.7 in) in diameter, is diagnosed in a 69-year-old woman. Considering the size of the growth, the prognosis is very unfavorable = attack against the abdomen. The patient feels threatened by the gigantic tumor in her abdomen > growth of cells in the peritoneum = peritoneal cancer. Three weeks later, as the tumor is removed, the surgeons find a number of stipple-shaped mesotheliomas. (Archive B. Eybl) |
| Conflict-active | Conflict–active Cell proliferation in the peritoneum, growth of small or flat mesotheliomas, depending on whether the person feels attacked over the whole abdomen or only at a certain spot. |
| Bio. function | Strengthening and thickening of the peritoneum to fend off attacks better. |
| Repair phase | Tubercular–caseating degradation along with fever, night sweats or encapsulation of the tumor if no suitable bacteria are present, development of abdominal fluid (ascites), especially with syndrome. Repair phase doesn’t automatically mean that “everything’s okay,” because the conflict may be persistent and the repair phase pain could become problematic due to its intensity. After the healing is complete, calcium deposits and scarring may remain. |
| Repair crisis | Chills, intense pain. |
| Questions | First determine if it is conflict-active or in the repair phase. Real attack to the abdomen? (Accident, blow/punch, OP, severe abdominal pain like a bilious attack)? Imagined attack? (Diagnosis, thoughts about if one may have an intestinal tumor or not)? Substitute conflict? (E.g., sympathy with a loved one who has an abdominal disease). Why does it affect me so much? Which family conditioning plays a role? |
| Therapy | Identify the conflict and conditioning and, if possible, resolve them in real life should they still be active. Understand the connections. Guiding principles: “I am safe. I am protected.“ “Everything is going to be all right again.“ “I know the connections, so this diagnosis cannot shake me.“ In CM, this condition is treated with an OP, chemotherapy and radiation for about three months of life extension. Right after the surgery, mesothelioma usually grow back in the surgery wound. In our view (and “from the perspective of the peritoneum“), this is understandable, because the surgery represents a renewed attack. > Due to their low chances of success, these CM therapies are not recommended. |
Inflammation of the peritoneum (peritonitis)
CM distinguishes between primary (the peritoneum is the source of the inflammation) and secondary (surrounding organs, e.g., intestines are the source of the inflammation) peritonitis. If primary peritonitis: Same SBS as above.
| Example | • A 35-year-old, right-handed man is sitting in the passenger seat next to his girlfriend, as she drives through an intersection with a green light. At this moment, a vehicle coming from the right crashes into the passenger side of the small car. The patient feels an impact from the side against his abdomen. The side airbag opens = attack conflict against the abdomen. He is brought to the hospital in an ambulance. Twenty-four hours after the accident, he experiences a strong pain. His abdomen is very hard and very sensitive to pressure = peritonitis. Forty-eight hours after the accident (the second day in the hospital), the abdomen of the athletic patient swells up into a big hard ball. The patient: “It was as if I were pregnant.“ = repair phase – ascites – exsudative peritoneal effusion. His swollen belly remains with him for two days and then he slowly urinates the fluid away and his pain subsides. (Archive B. Eybl) |
|---|---|
| Phase | Repair phase: Inflammation of the peritoneum, tumor-degradation via bacteria, fever, night sweats. The acute peritonitis has a serious set of symptoms: abdominal pain, “hard as a board“ peritoneum, acute pain in the repair phase crisis. |
| Therapy | The conflict is resolved. Support the healing process. Slight inflammation: Cannabis oil, cold brine or curd cheese compresses, enzyme preparations, Schuessler Cell Salts: No. 3, lymph drainage massages (see p. 68). If severe, generalized peritonitis, CM does the following: surgical removal of inflamed tissue and pus. They then rinse the abdominal cavity (peritoneal lavage). Subsequently, the patient needs intensive care with antibiotics and pain-killers. Whether these drastic measures are actually necessary, I do not know. Decide on a case-by-case basis. |
Ascites (exsudative ascites)
Ascites is when there is fluid in the peritoneal cavity. Ascites can form during the inflammation (repair phases) of any abdominal organ, even the bones, in conjunction with syndrome (= transudative ascites).
A swelling of the liver can mimic ascites.
Pronounced ascites occur in a peritoneum SBS + syndrome (= exudative ascites). See also p. 277.
The Same SBS as above (see: p.259), but with syndrome as well:
| Example | A patient is diagnosed with cancer of the liver and a surgery date is set = attack-to-the-abdomen conflict. The surgery is postponed 4-6 weeks in order to carry out pre-operative examinations. During the surgery, the abdomen is found to be “full of metastases“ = cell proliferation in the peritoneum (peritoneal mesothelioma). (See Dr. Hamer, Goldenes Buch Bd. 1, p. 348) A 55-year-old patient decides to have liposuction on her abdomen, because her husband has been criticizing her fat belly. When she sees the long needle poking around in her abdomen, she feels like she is being attacked. Mesotheliomas develop on the four spots where the needle was inserted. (See Claudio Trupiano, thanks to Dr. Hamer, p. 207) |
|---|---|
| Phase | Repair phase: A reduction of the mesothelioma goes hand-in-hand with the production of fluid. This prevents adhesions, since everything is “swimming“ in ascites > enlarged abdomen with weight gain, severe ascites with syndrome. Possibly recurring–conflict. |
| Therapy | The attack conflict is resolved. Support the healing. Resolve any refugee conflict (kidney collecting tubules). Tea: nettle, horsetail, goldenrod, sage. Normal drinking, little salt (whole salt), no pork. Lymphatic drainage, saltwater baths, enzyme preparation. Breathing exercises. If necessary: pain medication. Avoid punctures if possible or slowly lengthen the intervals between treatments. For chronic ascites, possibly implant a self-operated catheter. For treating loss of protein due to puncture > intake of biologically valuable proteins, such as eggs, curd cheese, protein 88, possibly also albumin infusions. |
1 See Dr. Hamer, Charts pp. 48, 53
Cancer of the inner navel1
In our developmental history, the inner part of the navel arose from the so-called cloaca. Birds and reptiles have no separate exits for feces and urine like most mammals; rather, they have a joint opening for everything. Even their sex organs open into the cloaca.
| Conflict | Chunk conflict (see explanations p. 15, 16), not being able to get something out (= elimination conflict). |
|---|---|
| Examples | A woman notices that her husband is drunk again. = Conflict, not able to eliminate the alcohol. An 11-year-old boy has a 9-year-old sister. His conflict is that his sister still wets her bed = substitution conflict, not eliminating (correctly). When his sister is finally “dry,“ his navel begins to leak fluid = repair phase, degradation of the navel tumor. (See Ursula Homm, Lebensmittelheilkunde, p. 44) |
| Conflict-active | Conflict–active Increase in function or growth of a compact cauliflower-shaped tumor (adeno-ca) of secretory quality or a flat-growing cancer of absorptive quality. |
| Bio. function | Improvement of excretion. |
| Repair phase | Normalization of function, tubercular-caseating degradation of the tumor via fungi or bacteria. |
| Questions | What can’t I eliminate? What do I want to be rid of? (For me or perceived as a substitute for someone else). Why did that appear in my life? Was it a message for me? Which familial conditioning sensitized me for the conflict? |
| Therapy | Identify the conflict and conditioning and, if possible, resolve them in real life if still active. OP if necessary. |
1 See Dr. Hamer, Charts p. 28
Cancer of greater omentum (omentum majus), cold abscess in abdominal cavity1
Tumors of the greater omentum are largely unknown in CM. Again, Dr. Hamer discovered something new.
| Conflict | Conflict relating to the abdomen. |
|---|---|
| Example | ➜ A large tumor is discovered in someone‘s abdomen. |
| Conflict-active | Cell proliferation in the greater omentum, growth of a mesothelioma. |
| Bio. function | 1. Providing more fluid for a good lubrication of the abdominal viscera. 2. “Wrapping up” of the inflamed abdominal organs through the intrinsically mobile greater omentum. |
| Repair phase | Tubercular-caseating degradation of the tumor, often along with adhesions. The encapsulation of centers of inflammation in the abdomen are also known as “cold abscesses“ in CM. |
| Questions | Determine if the conflict is active or in the repair phase based on the symptoms. What happened with my own abdomen or the abdomen of a loved one? (OP, injury, bad diagnosis or fear thereof)? Am I carrying something from the family (familial solidarity)? Are there unresolved issues in the family with relation to the abdomen/digestion? |
| Therapy | Determine the conflict and conditioning and, if possible, resolve them in real life if still active. |
1 See Dr. Hamer, Charts pp. 48, 53
Abdominal wall hernia, inguinal hernia, umbilical hernia
90% of hernias occur in men. This is because, in the large inguinal canal, there is a weak spot in the male abdominal wall. This canal can become a hernial orifice and abdominal contents (intestinal loop) can force its way out.
| Conflict | Self-esteem conflict: too much pressure, having to carry too much, always pushing and pressing. In the case of children, it is always a substitution conflict (check the parents). |
|---|---|
| Conflict-active | Conflict–active Unnoticed cell depletion in tendon sheets or in connective tissue of the abdominal wall. Prolonged conflict activity can cause tendons to be pushed to the side through increased abdominal pressure (long-term expansion of intestine from gas, straining during bowel movements, lifting, coughing) and a hernial orifice or a hernial sac develops. |
| Repair phase | Recovery only when the hernial orifice rests, closed, for a few months. |
| Bio. function | Strengthening the abdominal wall in order to be able to withstand more pressure. |
| Questions | When was the hernia noticed? (Conflict-active phase at least some weeks before). Which pressure from outside was I unable to withstand? Did I put myself under pressure? Tendency toward hernias in the family? (Yes > work out the family tendency) When did everything become so difficult? |
| Therapy | Identify the conflict and conditioning and, if possible, resolve them in real life. Guiding principle: “I let it flow and it’s easy going.” Comfrey, sanicle internally and externally. Improve nutrition so that no intestinal gases develop and the intestine isn’t burdened. Wear an athletic supporter for a few months. The hernial sac must never fill during this time. OP if all else fails. |
All experience reports on the organ system “Peritoneum, Navel, Gr. Omentum and Abdominal Wall” from the International Report Archive:
| Author | Title and Overview | Keywords | ||||
|---|---|---|---|---|---|---|
 | 2025/10/24   A mother's peritonitis and pancreatitis following her newborn son's serious illness. | Tackling aggression, attacking the abdomen | ||||
 | 2015/01/01 Here is a list of other sources where experience reports with the 5BN can be found, e.g. to:: Bursitis, conjunctivitis, rheumatism, diabetes, hay fever, psoriasis, bedwetting, stuttering, oceans, aggressive constellation, endometrial CA, cervical cancer, shingles, tinnitus, toothache, heart attack, high blood pressure, colic, slipped disc, knee pain, leukemia, bone cancer, voice gone, stomach pain, hives, Epilepsy, intolerances, Crohn's disease, skin rash, facial paralysis, hiccups, anorexia, bronchitis, corneal inflammation, migraine, thyroid cyst, aphthae, osteolysis, gastritis, rectal spasms, milk duct carcinoma, allergies, hepatic coma, gray hair, nail fungus, heartburn, nasal polyps, caries, heart attack, ankylosing spondylitis, melanoma, psoriasis, water belly, hailstones, prostate, . .. |